
An Architecture in Disguise as Deficit: Rethinking ADHD in the Age of Overstimulation
- Derek Li

- Jan 29
- 5 min read
Look at this image.

If you asked a city planner to fix traffic here, they wouldn’t say, “The problem is that there are too many roads.” They would say, “This is a high-throughput system designed to handle massive complexity.”
Yet when we encounter a brain wired in much the same way, firing on all cylinders, processing multiple streams of information at once, we don’t call it a supercomputer.
We call it a deficit.
In recent years, ADHD diagnosis and recognition have risen sharply. In the United States, an estimated 15.5 million adults (6.0%) reported a current ADHD diagnosis in 2023 (CDC, 2024). Among children, national survey data show that approximately one million more had ever received an ADHD diagnosis in 2022 compared with 2016 (Danielson et al., 2024).
Are we witnessing a sudden failure of the human brain?Or are we the first generation trying to make Ferrari engines behave like school buses?
It may be time to rethink ADHD not as a bug, but as a misunderstood architecture.
1. Two Very Different Ways a Brain Can Overheat

Before we romanticize the supercomputer, we need to clear up a critical confusion in
modern mental health discourse. Not every “busy” brain is built the same way. Today, two distinct phenomena are often grouped under the same label: neurodevelopmental ADHD and stress- or trauma-related attentional dysregulation (Figure.1)
They can look similar on the surface.They are not the same underneath.
Trauma- and Stress-Related ADHD-Like Patterns
In some individuals, attention difficulties arise primarily as an adaptation to prolonged stress or trauma. Research in developmental neuroscience and psychotraumatology has long shown that chronic stress and early adversity can alter attention, executive function, and threat-monitoring systems (McEwen & Morrison, 2013; Teicher & Samson, 2016).
These patterns are often associated with:
Chronic stress
Developmental or relational trauma
Attachment disruption
Persistent hypervigilance
The brain adapts by:
Remaining on high alert
Scanning constantly for threat
Struggling to sustain attention in contexts that feel “safe” but unfamiliar
Here, attention difficulties are defensive, not architectural.The brain is not failing to focus. It is prioritizing safety over efficiency.This system does not need optimization.It needs regulation, predictability, and safety.
Importantly, trauma-related dysregulation and ADHD frequently co-occur, complicating diagnosis and treatment and underscoring the need for careful, individualized assessment (Ford & Courtois, 2021).
The Neurodevelopmental “Supercomputer”
There is, however, another profile entirely.
Neurodevelopmental ADHD is associated with early-emerging differences in brain networks involved in attention, reward processing, and executive control (Castellanos & Proal, 2012; Nigg, 2017). These differences are not inherently pathological.
This brain processes information rapidly, forms wide associative networks, and often performs best in environments rich with novelty, complexity, and meaning.
This is not a damaged system.It is a high-speed architecture.
Often characterized by:
Parallel processing
Pattern recognition
Divergent thinking
Intense, immersive flow states
Placed in linear, repetitive, low-stimulation environments, this brain appears restless and unfocused. But that appearance is misleading. The difficulty is not a lack of capacity. It is a mismatch between architecture and environment.
It is a supercomputer trying to survive on dial-up.
2. The Plot Twist
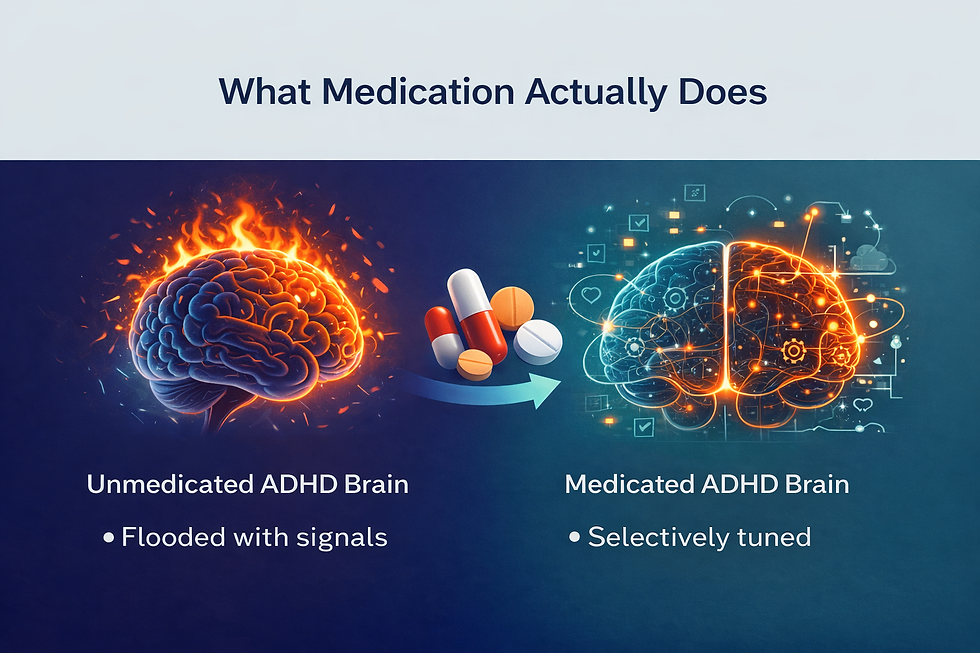
For decades, the dominant explanation was simple:“You have an attention deficit. Take a stimulant to fix your attention.”
Recent neuroscience has complicated that story.
A large-scale neuroimaging study published in Cell in late 2025 suggests that stimulant medications such as methylphenidate and amphetamines do not primarily exert their effects by strengthening canonical attention-control networks (Kay et al., 2025).
Instead, these medications appear to act largely on arousal and reward-related brain systems, including networks involved in wakefulness and motivational salience (Kay et al., 2025; NIH, 2025).
In practical terms, stimulants often make low-interest tasks easier to initiate and sustain by increasing alertness and perceived reward.
They do not repair a broken steering wheel.They increase fuel and engine responsiveness so the system is less likely to stall.
This reframes ADHD in an important way.
For many individuals, the primary bottleneck is not intelligence or attentional capacity.It is arousal regulation, reward sensitivity, and task salience, long recognized as central features of ADHD neurobiology (Volkow et al., 2011; Sonuga-Barke, 2015).
The ADHD brain is often capable of deep, sustained focus when engagement is high. It simply struggles to idle in low-stimulation conditions without meaningful incentive.
3. From Symptom Control to System Design
What begins to emerge from this shift is not a new “treatment,” but a different way of seeing.
If attention difficulties are not simply deficits to be suppressed, but signals of a system operating outside the conditions it was designed for, then the question itself changes. It moves from How do we force this mind to behave? to What would it look like to design around how it actually works?
Research across neuroscience and psychology increasingly suggests that performance in ADHD is highly context-dependent, shaped by the interaction between arousal, reward, task structure, and environment (Sonuga-Barke, 2015; Volkow et al., 2011). When these elements are aligned, many individuals with ADHD demonstrate sustained focus, creativity, and high-level problem solving. When they are not, the system destabilizes.
Some nervous systems function as high-throughput, high-pressure architectures. They perform best in conditions of engagement, meaning, and complexity, and they struggle when forced into prolonged trickle. When such systems are blocked or chronically mismatched to their environment, they do not slow down gracefully. They overheat. They fragment. They burst.
What we often label as symptoms may, in this light, be less about internal failure and more about systemic friction.
A systems-oriented lens asks how arousal, reward, rhythm, and environment interact, and how relatively small changes in context can dramatically alter performance without overriding the system itself. This perspective complements pharmacological approaches, which primarily support arousal and motivational salience, by addressing the broader conditions under which the nervous system operates (Kay et al., 2025; NIH, 2025).
Whether or not we give this way of thinking a name, the principle remains the same: move beyond symptom control and toward system design.

We are not broken.We are bio-conductive.
Architectures shaped for complexity, still learning how to run powerful software without overheating the hardware.
And perhaps the work ahead is not simply to survive the pressure, but to learn how to let it flow.
References
Castellanos, F. X., & Proal, E. (2012). Large-scale brain systems in ADHD. Trends in Cognitive Sciences.
Centers for Disease Control and Prevention. (2024). Prevalence of ADHD among U.S. adults. MMWR.
Danielson, M. L., et al. (2024). Trends in ADHD diagnosis among U.S. children. Journal of Clinical Child & Adolescent Psychology.
Ford, J. D., & Courtois, C. A. (2021). Complex PTSD and developmental trauma.
Kay, B. P., et al. (2025). Stimulant medications affect arousal and reward networks. Cell.
McEwen, B. S., & Morrison, J. H. (2013). The brain on stress.
National Institutes of Health. (2025). How ADHD medications influence alertness and motivation.
Nigg, J. T. (2017). Attention-deficit/hyperactivity disorder and adverse outcomes.
Sonuga-Barke, E. J. S. (2015). The dual pathway model of ADHD.
Volkow, N. D., et al. (2011). Motivation deficit in ADHD.

Comments